Biomarker confirmation of AD may improve disease care
Your patient's initial cognitive complaint or observed impairment may be your trigger to detect, assess, and diagnose early-stage AD. A key part of the process can be biomarker confirmation to support the diagnosis.1-4
The path to diagnosing early-stage AD1-6
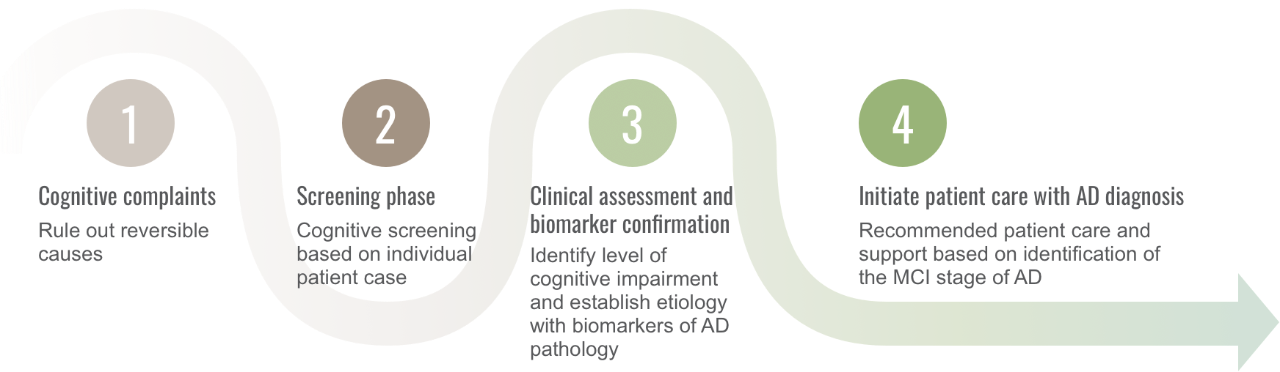
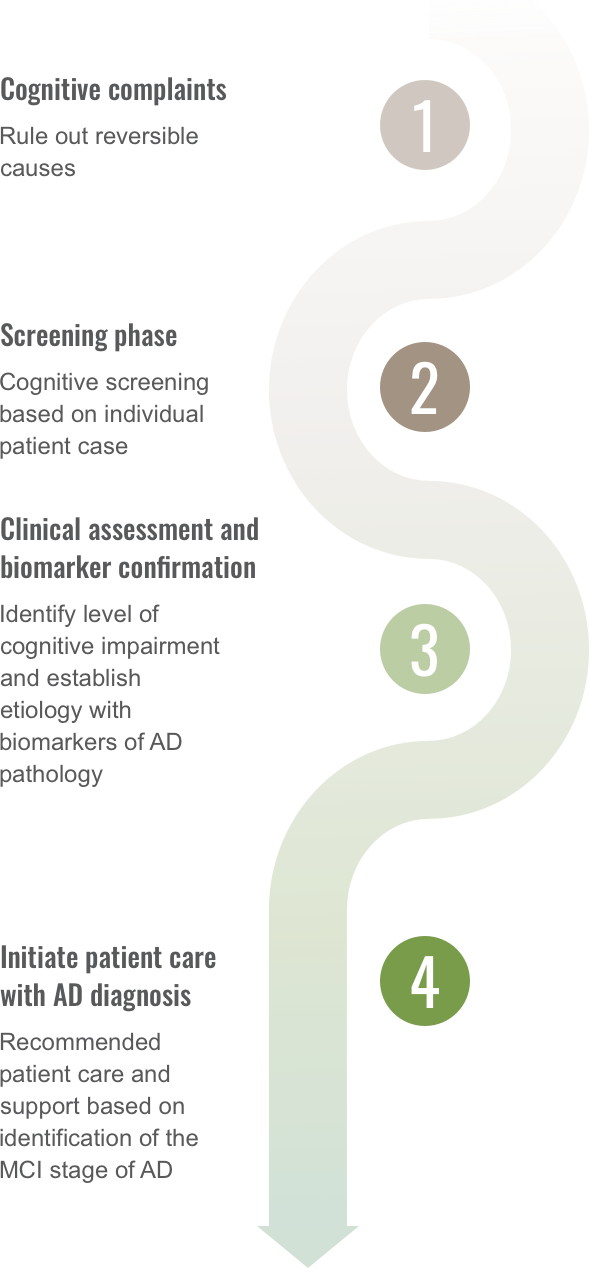
Potential utility for biomarker confirmation
According to International Working Group (IWG) recommendations, a diagnosis of AD requires a clinical evaluation and confirmation of AD pathology. The diagnostic value of AD as the cause of MCI provides the clinician an opportunity to initiate patient care.7
Biomarkers focused on AD
There are a wide variety of biomarkers available for neuropathological diagnosis of AD. For instance, positron emission tomography (PET) imaging and cerebrospinal fluid (CSF) tests can determine whether amyloid beta (Aβ) and tau pathology are present in the brain, biomarkers that are currently considered valid proxies for neuropathologic changes of AD.8
Many other biomarkers that are commonly used in research are non-specific indicators of neuronal damage. And while magnetic resonance imaging (MRI) is widely available and recommended as part of the diagnostic criteria, especially to rule out other possible causes, it lacks molecular specificity and cannot confirm AD pathology.9
Methods of evaluating biomarkers
PET Imaging
PET imaging uses radiotracers to bind to amyloid plaques or tau in the brain. The amyloid PET scan10:
- Offers high diagnostic accuracy and localized information10
- Provides a means to directly assess relative AD pathology in the brain10
- May be used to establish biomarker relationships with changes in cognition and neurodegeneration11
Amyloid PET provides an image of Aβ aggregation8,12

Images from Huang CC, et al, used under CC BY 4.0, https://creativecommons.org
/licenses/by/4.0/.
CSF Test
Obtained via a lumbar puncture, a single collection of CSF can be used to assess brain pathology and to measure Aβ and tau biomarkers.8,10
- Levels of Aβ in CSF are inversely related to the extent of cerebral Aβ deposits13
- CSF phosphorylated tau (p-Tau) is a biomarker of the abnormal pathophysiology specifically associated with neurofibrillary tangles in AD. It is not elevated in primary tauopathies, head injury, or stroke8
- CSF total tau is a biomarker of neuronal degeneration; it is not specific for AD8
- Ratios of CSF biomarkers, eg, Aβ42/Aβ40 or p-Tau/Aβ42, are more accurate indicators of clinical AD and have less variability in assays than CSF Aβ42 alone14,15
CSF is collected between the 3rd and 4th, or 4th and 5th vertebrae15,16
